Fibroliposarcoma and malignant melanoma
Identification and history
- Name: Boujee
- Report and medical history: canine, mixed breed; male, entire, 8 years old.
The patient was brought in due to recent loss of appetite and reduced activity for about 5 days. Occasional dysuria was also reported.
Diagnostics
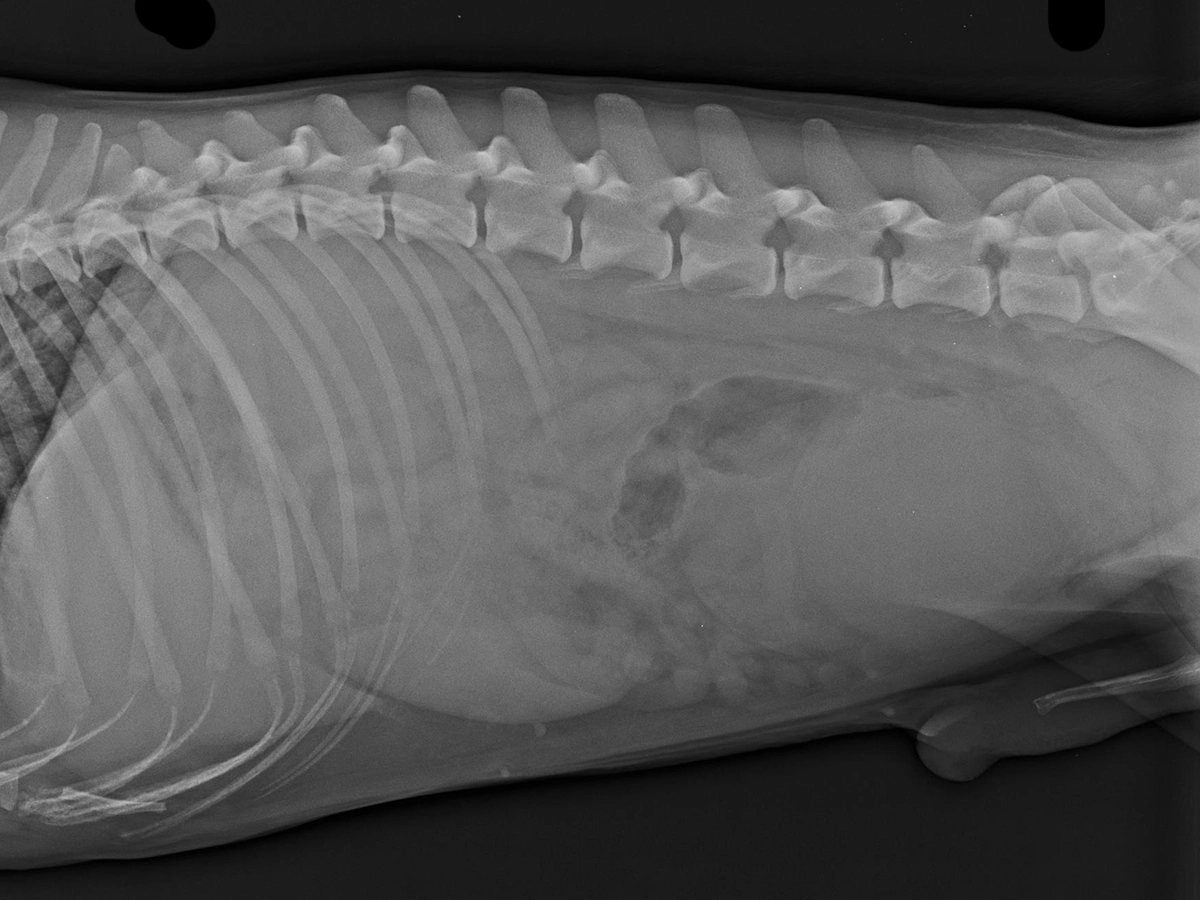
An orthogonal radiograph of the abdomen revealed a large, rounded, well-defined soft tissue opaque mass in the right caudoventral abdomen, superimposed with the urinary bladder on the lateral view. Overall, the serosal margin detail is reduced and there is a mild fluid streaking surrounding bladder and the described mass. Hematological examination revealed leukocytosis and elevated total protein
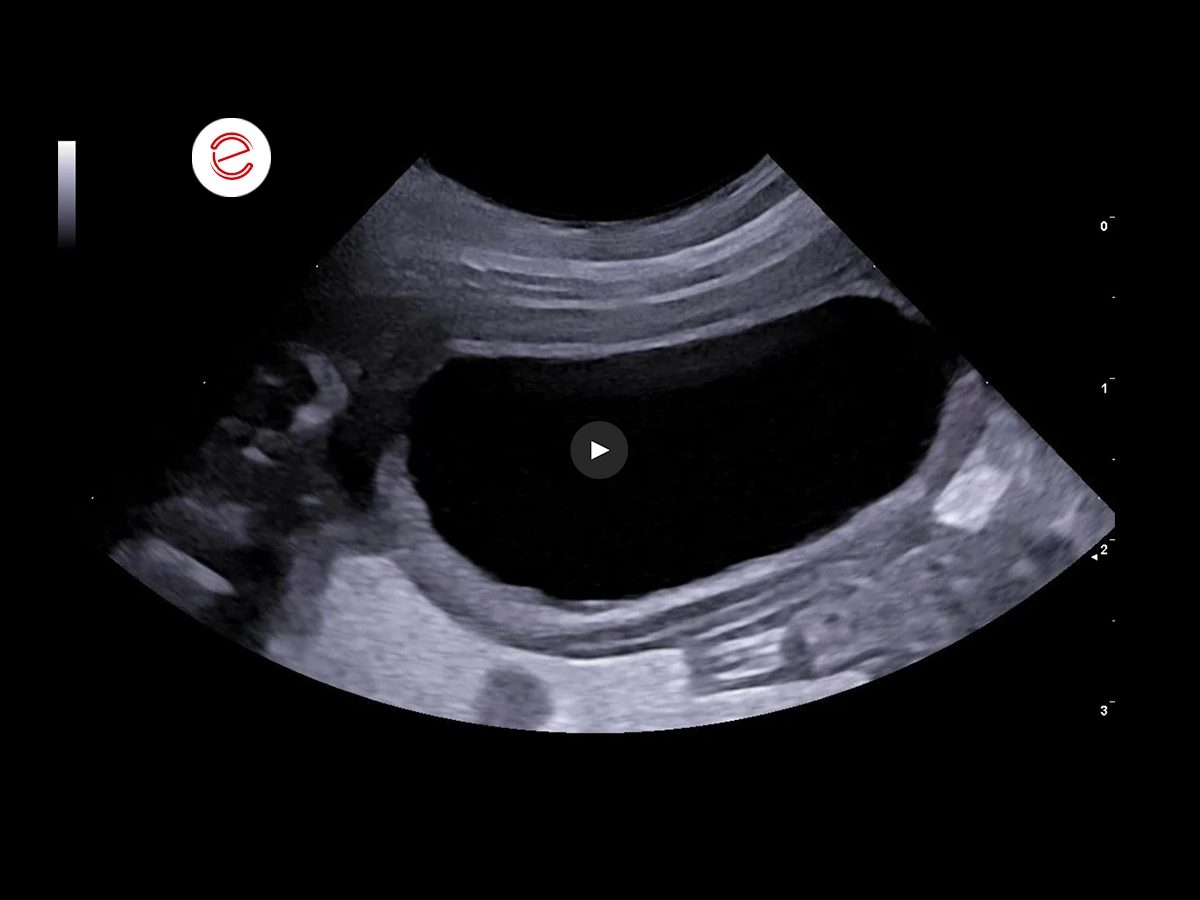
The urinary bladder is moderately filled with anechoic content. The wall is moderately thickened with mild irregularity of the apical bladder mucosa.
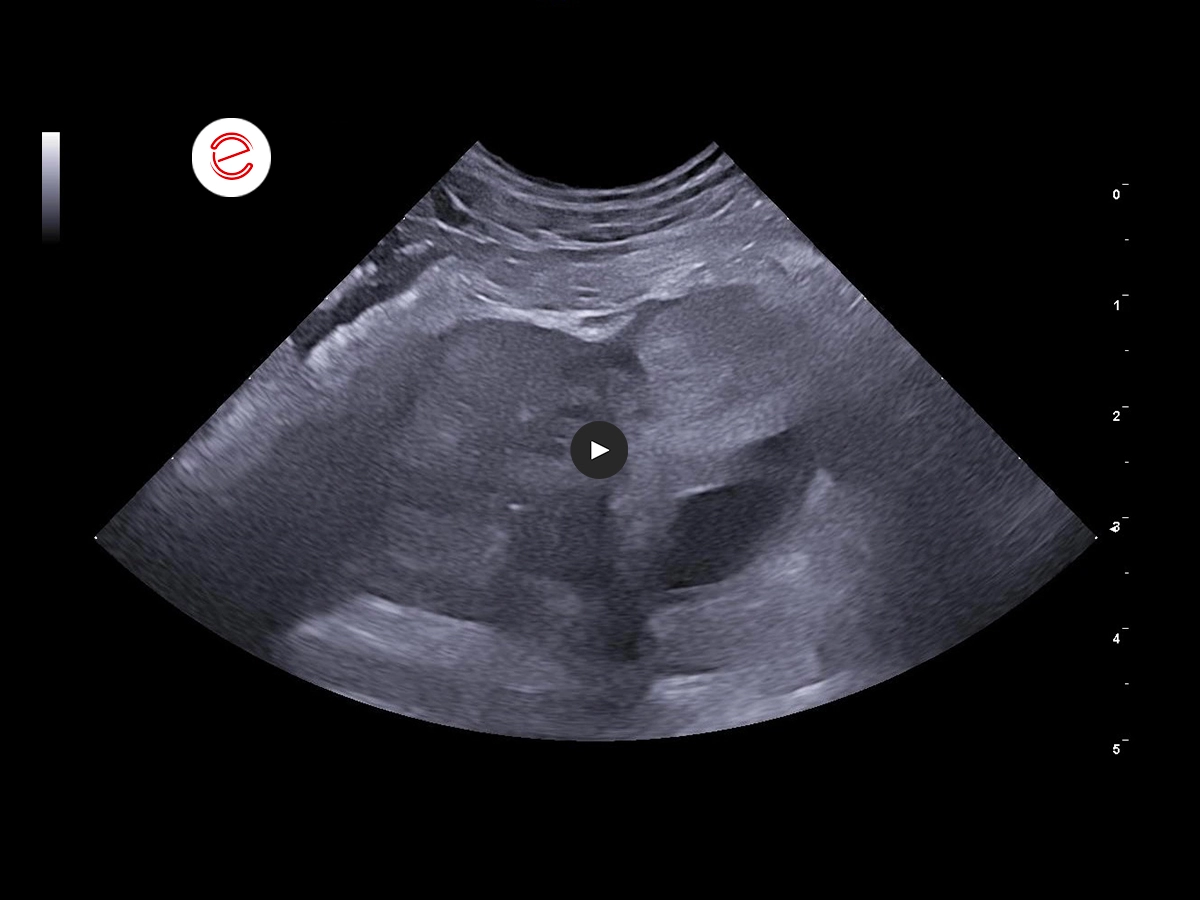
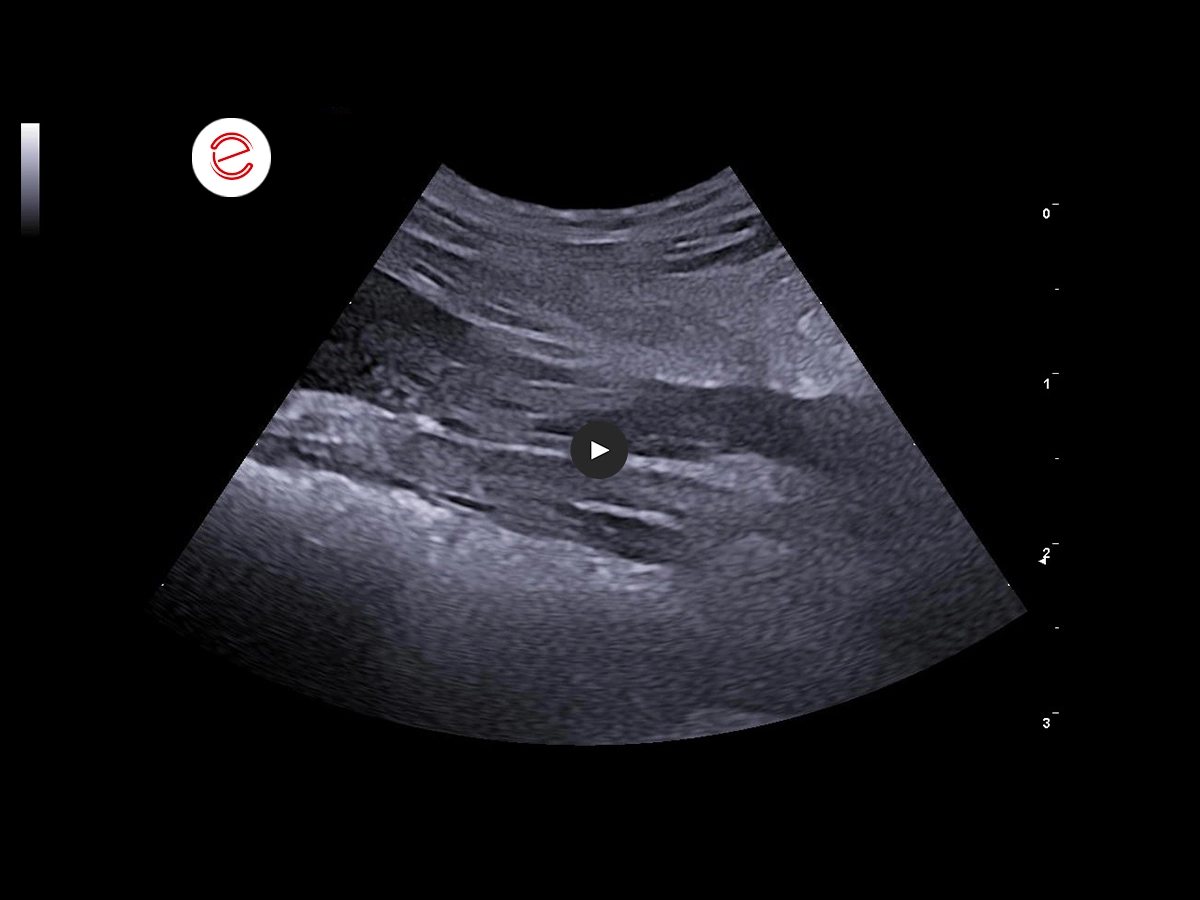
The prostate gland is asymmetrically enlarged with a inhomogeneous echotexture and hyperechoic echogenicity. There are well-defined, irregularly shaped intraparenchymal cysts with anechoic contents in the left prostatic lobe.
The periprostatic fat is hyperechoic. There is pain on palpation and during examination of this area.
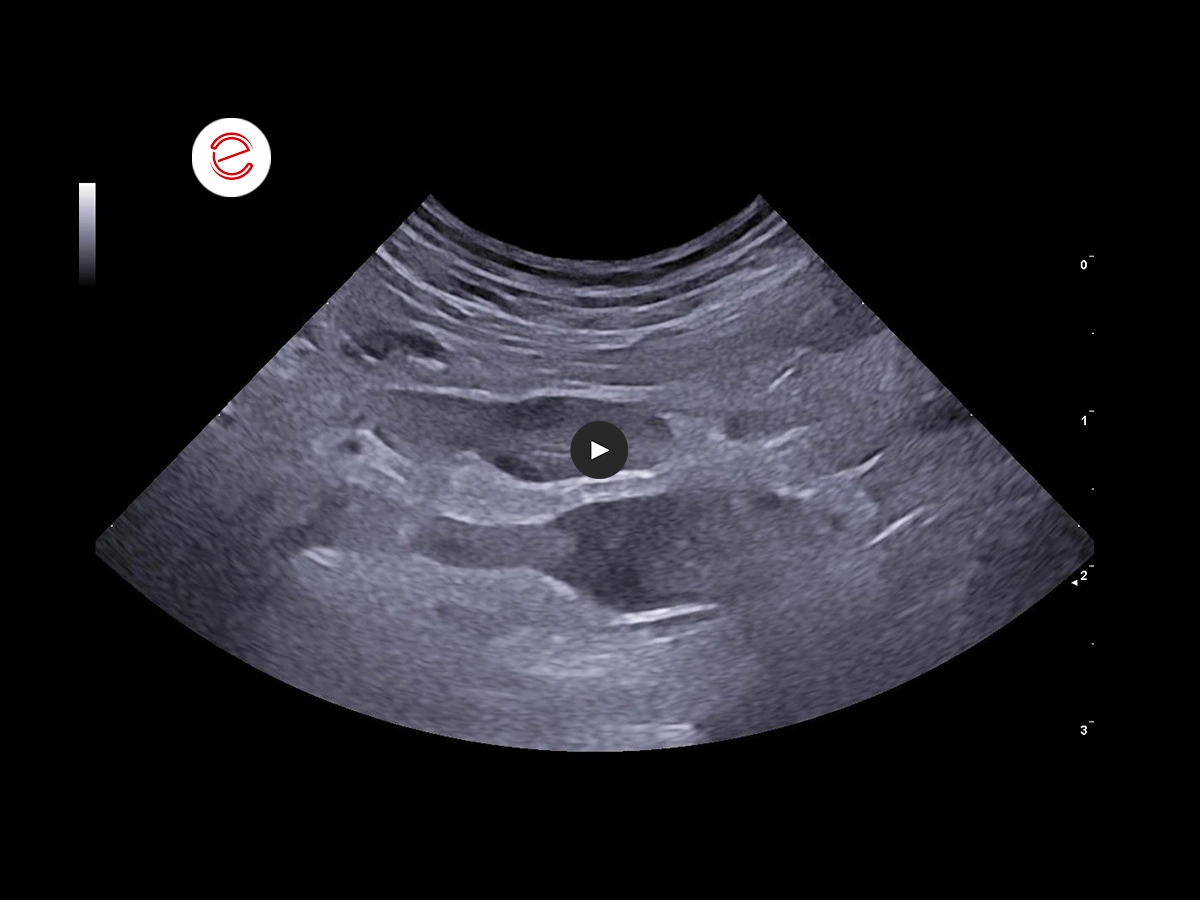
There is a smaller intraparenchymal cyst in the right lobe that communicates with a large intra-abdominal cystic structure that extends cranially in the mid-abdomen.
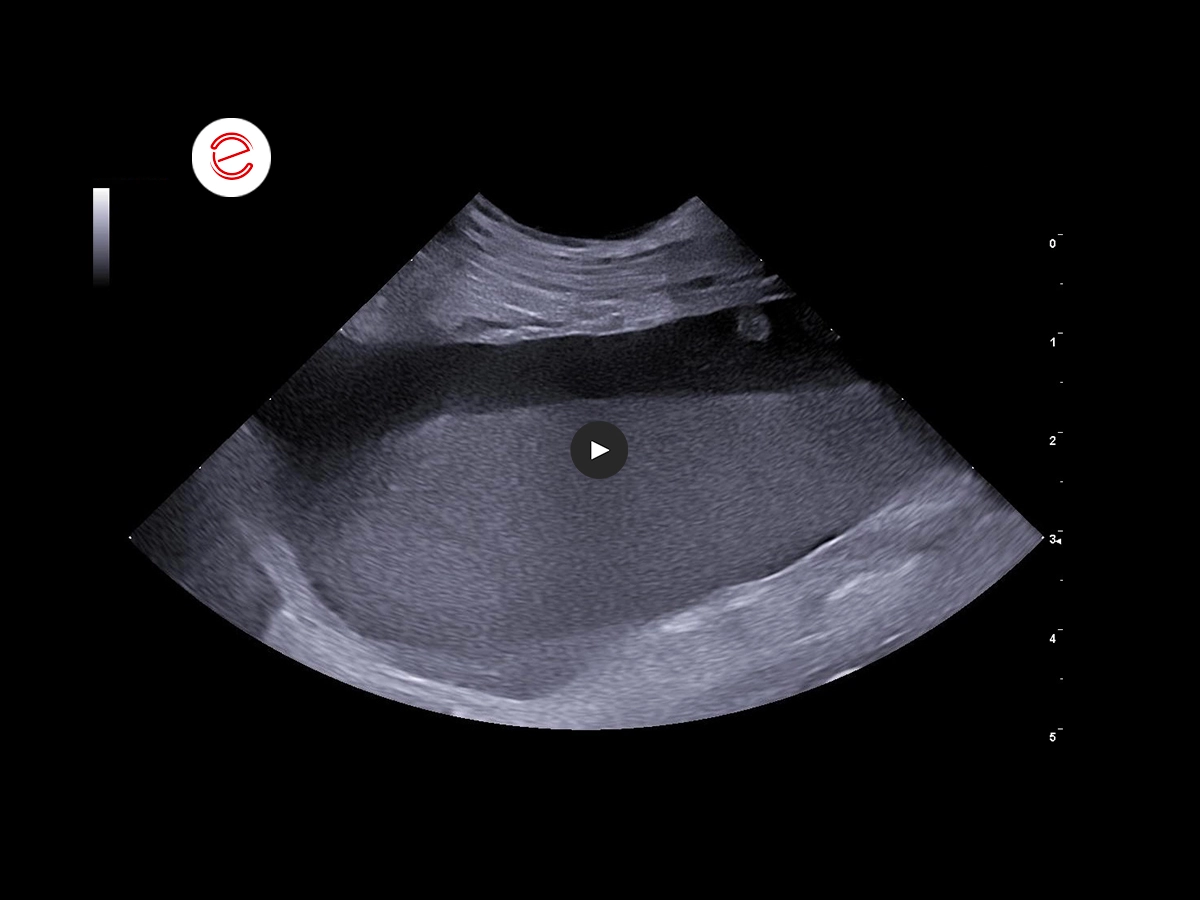
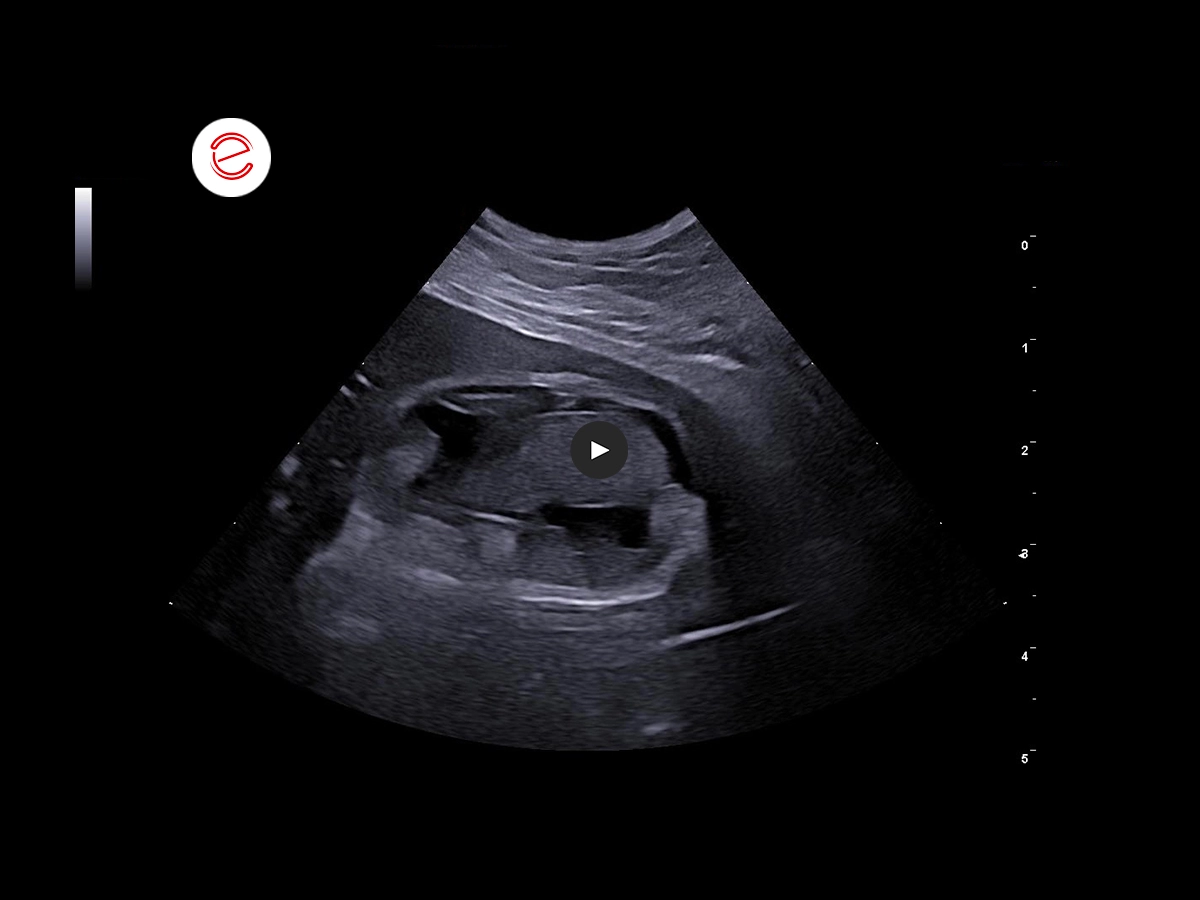
The large cystic structure contains echogenic materials with visible sedimentation within the dependent lumen. There is generalized increased in echogenicity of the surrounding mesentery. There are membranous irregular intraluminal echoes in the dorsal wall extending to the cranioventral end.
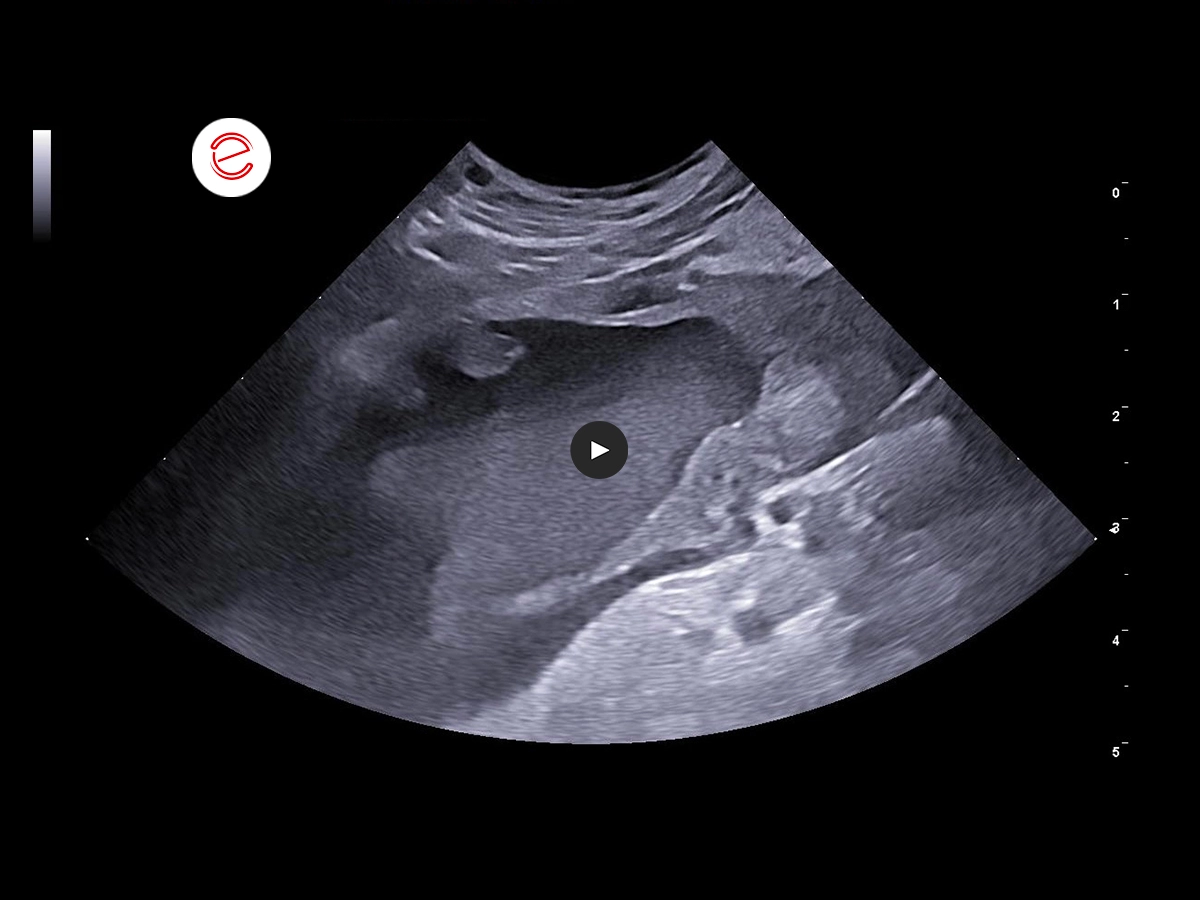
In the area of the trigone, dorsal to the urinary bladder and ventral to the descending colon, there is a hypoechoic tubular structure measuring about 3-4 mm in diameter. A central echogenic area is visualized in the transverse section. The cranial end of this tubular structure was not identified.
The medial iliac lymph nodes are moderately enlarged with ill-defined hypoechoic to anechoic areas and irregular margins.
The gallbladder is normal in size with moderate echogenic non-shadowing, non-gravity-dependent contents. The wall appears diffusely thickened. There is no biliary dilation.
Cytological analysis of paraprostatic fluid
The stained slides reveal a moderately cellular smear, which is primarily composed of a mixture of normal and occasionally crenated red blood cells, with a marked proliferation of neutrophils and degenerate neutrophils. Rarely interspersed among these cells are atypical, medium-to large-sized, moderately pleomorphic neoplastic cells that display a variable amount of amphophilic to lightly basophilic cytoplasm, lacking distinct cellular borders.
These cells possess large, moderately pleomorphic, round-to-ovoid nuclei that are often hyperchromatic, containing coarse chromatin granules and a variable number of single distinct nucleoli. Anisokaryosis and anisocytosis are mild to moderate, and mitotic figures are rare. The nuclear-cytoplasmic ratio of the neoplastic cells is high, ranging from 0.6 to 0.8.
Diagnosis
Findings suggest a benign neoplastic process with concurrent inflammation.
Treatment
Exploratory laparotomy was performed after three days of hospitalization and medical management. At surgery, a uterus-like smooth muscle structure was identified at the location described on ultrasound findings. The body of this structure terminates in the prostate while both horns were found to extend towards their respective inguinal canals. The paraprostatic cyst was intimately associated with the right lateral wall of the urinary bladder from which it was partially separated by careful dissection. Cyst drainage and omentalization was performed. Sections of the resected cyst wall were submitted for histopathological analysis.
The patient was discharged after three days of hospitalization and the clinical signs resolved.
Histopathological findings
The tissue sections present streams of large plump fibroblasts showing moderate anisocytosis and anisokaryosis with large pleomorphic nuclei and distinct nucleoli interspersed with varying clusters of poorly differentiated adipocytes, some with scant to abundant cytoplasmic fats deposits. The neoplastic adipocytes show mild to moderate anisocytosis and anisokaryosis with large pleomorphic nuclei and prominent nucleoli. Large areas of necrosis with moderate to marked neutrophilic infiltration. Sparsely distributed large melanocytes with abundant intracytoplasmic melanin granules seen in some areas of the tissue section and intravascular infiltration. The neoplastic melanocytes show moderate anisocytosis and anisokaryosis with pleomorphic nuclei mostly obscured by melanin granules.
Vascularization is moderate; mitotic activity is moderate (10-12/10 hpf).
Diagnosis
Mixed Tumor (Fibroliposarcoma and Malignant Melanoma).
Images were acquired using the MyLab™FOX.
Conclusions and treatment
The changes observed in the prostate gland, localized steatitis, pain during probe manipulation and possible reactive medial iliac lymph node are highly suggestive of prostatitis with concurrent benign prostatic hyperplasia. The large intraabdominal solitary cyst with direct communication to the prostate is characteristic of a paraprostatic cyst. The cystitis should be considered with mucosal irregularity of the apical urinary bladder. For further investigation, ultrasound-guided needle aspiration was performed for urine and paraprostatic fluid analysis. One of the conditions associated with paraprostatic cyst is uterus musculinis. The observed tubular structure bounded dorsally by the colon and ventrally by the urinary bladder is possibly a derivative of the Müllerian duct. The heterogeneity of the medial iliac lymph nodes can be due to reactivity to underlying prostatic abnormality, paraprostatic cyst or due to developing neoplastic changes. The findings on the gallbladder is suggestive of biliary sludge or a developing gallbladder mucocele.
Reynaldo Buan Jr., DVM, MSc
Buan Veterinary Practice
Pampanga, Philippines

MyLab is a trademark of Esaote spa.
Technology and features are device/configuration-dependent. Specifications subject to change without notice. Information might refer to products or modalities not yet approved in all countries. Product images are for illustrative purposes only. For further details, please contact your Esaote sales representative.
Other canine clinical cases you may be interested in
Discover the challenges faced, the examinations performed, the solutions adopted, and the treatments recommended.

MAY 2025
Adrenomegaly and bilateral nephropathy
University Veterinary Hospital, Department of Diagnostic Imaging, University of Milan, Lodi.

MARCH 2025
Adrenal tumors
Carmelo Marco Bruno, DVM, specialist in pathology and clinic of companion animals, accredited with FSA and BOL

MAY 2024
Synovial Sarcoma
Daniel Sáez, DVM
Centro de Diagnóstico Veterinario Vetpoint®, Chile
